TeleportScienceNav
Preanalytical Phase
Due to its ease of access and its central role in biological functions, much emphasis has been placed on analyzing blood specimens for biomarker discovery. The main clinical blood specimens are plasma and serum. One critically important, and often underestimated factor modulating the likelihood of success in discovering relevant biomarkers in blood specimens are the procedures used in sample collection and specimen generation.
This preanalytic phase can significantly alter the results derived from the analysis of blood-derived samples by introducing unwanted systematic biases. The preanalytical phase comprise the processes prior to the actual analysis of the sample and include steps needed to obtain the primary sample (e.g. blood) and to obtain the analytical specimen (e.g. plasma, serum, cells). Standardization of blood sample collection is a prerequisite to avoid systemic biases.
Awareness of clinical practices in medical laboratories and the current knowledge allow for identification of specific variables, that affect the results of a proteomic study. Knowledge of pre-analytical variables is a prerequisite to understand and control their impact.
This preanalytic phase can significantly alter the results derived from the analysis of blood-derived samples by introducing unwanted systematic biases. The preanalytical phase comprise the processes prior to the actual analysis of the sample and include steps needed to obtain the primary sample (e.g. blood) and to obtain the analytical specimen (e.g. plasma, serum, cells). Standardization of blood sample collection is a prerequisite to avoid systemic biases.
Awareness of clinical practices in medical laboratories and the current knowledge allow for identification of specific variables, that affect the results of a proteomic study. Knowledge of pre-analytical variables is a prerequisite to understand and control their impact.

PXBioVisoN Blood Collection Protocol:
Download an in-depth description and a protocol from our website
Platelet Poor Plasma
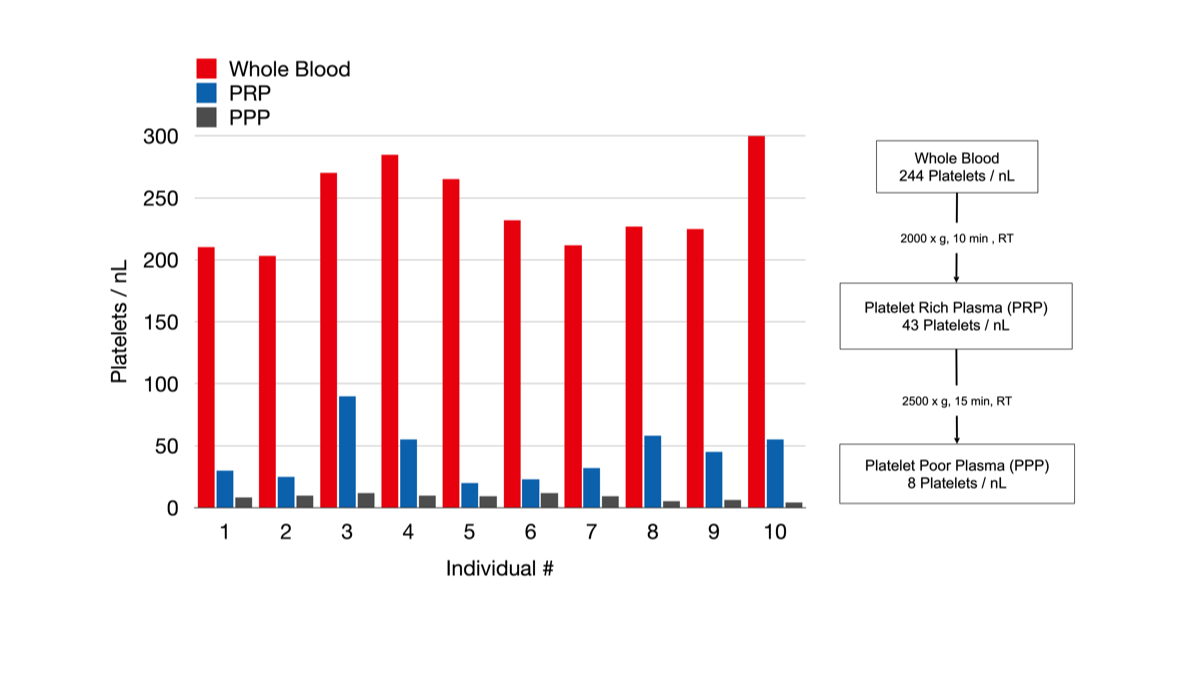
A quick separation of cells from the plasma is favorable, since cellular constituents may liberate substances that alter the composition of the sample. Generally, it is recommended that plasma and serum be centrifuged with 1300-2000x g for 10 min within 30 min from the collection of the sample. The temperature should generally be 15-24°C, unless recommended differently for distinct analytes like gastrin or A-type natriuretic peptide. Processing at 4°C appears to be attractive, because enzymatic degradation processes are reduced it low temperatures. However, platelets become activated at low temperatures and release intracellular proteins and enzymes, which affect the sample composition. Thus, processing at low temperatures is safe only after thrombocytes have been removed. Since one centrifugation step may be insufficient for depletion of platelets below 10 cells/L , a second centrifugation step (2500 x g for 15 min at room temperature) or filtration step may be required to obtain
platelet-poor plasma (PPP). This procedure is applicable only to plasma since the platelets in serum are already activated.
platelet-poor plasma (PPP). This procedure is applicable only to plasma since the platelets in serum are already activated.
Serum or Plasma ?
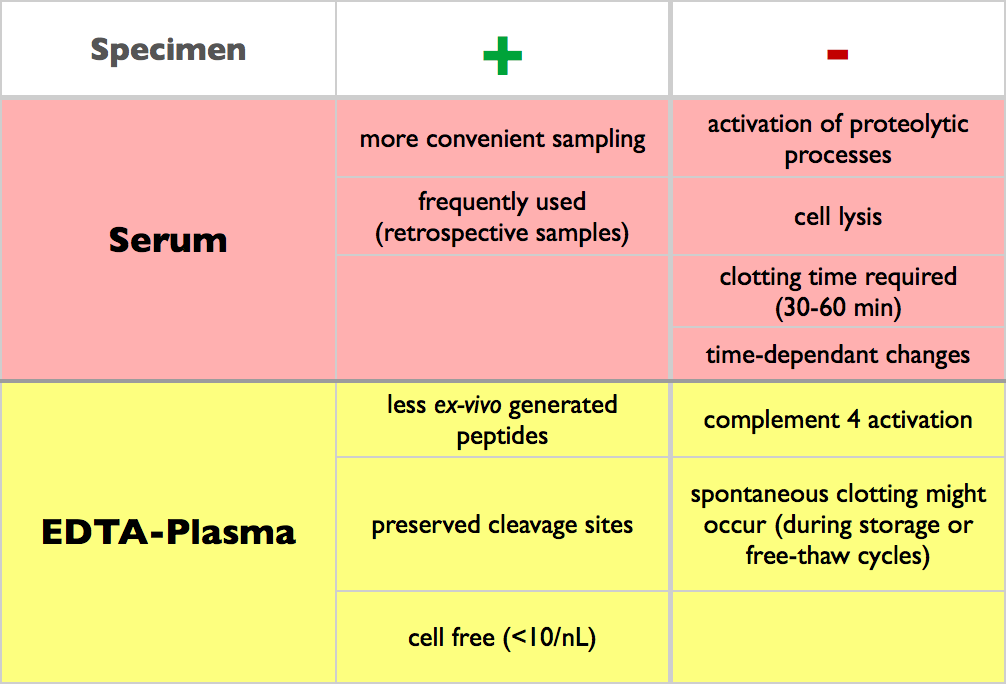
For Peptidomics® analyses EDTA plasma is the preferred specimen, since the proteolytic activity in comparison to serum is markedly reduced due to inhibition of ion-dependent enzymes via chelate formation. Avoiding ex-vivo degradation of proteins and peptides is beneficial, since the complexity of the resulting sample is reduced and for the analysis of in vivo protease cleavage sites it is mandatory to preserve the integrity of the peptidome.
Serum is one of the most frequently analyzed blood specimen. Generation of serum is time consuming and associated with the activation of coagulation cascade and the complement system. These processes influence the composition of the samples since they result in cell lysis (e.g. thrombocytes, erythrocytes). As a consequence the concentration of components in the extra cellular fluid such as aspartate-aminotransferase, serotonin, neuron-specific enolase and lactate-dehydrogenase are increased. On the other hand a fast degradation of analytes (e.g. hormones) may occur. On the proteomic level more peptides and less proteins are observed in serum when compared to plasma.
Consequently, the activation of clotting cascades necessary to generate serum can lead to artifacts. A reason to use serum as a specimen is based on the notion that the proteome or peptidome of serum may reflect biological events. Post-sampling proteolytic cleavage products have been proposed as biomarkers, and it has been further suggested that the serum peptidome is of particular diagnostic value for the detection of cancer. However, it has been reported that more protein changes occur in serum than in plasma. Thus, it can be expected that the reproducibility of such ex vivo proteolytic events is comparatively low.
Consequently, the activation of clotting cascades necessary to generate serum can lead to artifacts. A reason to use serum as a specimen is based on the notion that the proteome or peptidome of serum may reflect biological events. Post-sampling proteolytic cleavage products have been proposed as biomarkers, and it has been further suggested that the serum peptidome is of particular diagnostic value for the detection of cancer. However, it has been reported that more protein changes occur in serum than in plasma. Thus, it can be expected that the reproducibility of such ex vivo proteolytic events is comparatively low.
In contrast to serum Citrate and EDTA inhibit coagulation and other enzymatic processes by chelate formation with ions, thereby inhibiting ion-dependent enzymes. This is in contrast to heparin, which acts through activation of antithrombin III. The main concern associated with heparinized plasma for proteomic studies is that it is a poly-disperse charged molecule that binds many proteins non-specifically and may also influence separation procedures mass spectrometric detection of peptides and small proteins due to its similar molecular weight.
The sampling of plasma is less time consuming than the acquisition of serum. Separation of cells and the liquid phase can be performed subsequently to sample collection since no clotting time is required (30-60 min). In comparison to serum the amount of plasma generated from blood is approximately 10 to 20 % higher. Additionally the protein content of plasma is also higher than in serum, because of the presence of clotting factors and associated components. Furthermore, proteins may be bound to the clot, resulting in decrease of protein concentration during formation of the clot.
The sampling of plasma is less time consuming than the acquisition of serum. Separation of cells and the liquid phase can be performed subsequently to sample collection since no clotting time is required (30-60 min). In comparison to serum the amount of plasma generated from blood is approximately 10 to 20 % higher. Additionally the protein content of plasma is also higher than in serum, because of the presence of clotting factors and associated components. Furthermore, proteins may be bound to the clot, resulting in decrease of protein concentration during formation of the clot.
Protease Inhibitors
Protease inhibitors would be attractive, but commonly used protease cocktails may introduce difficulties due to interference with mass spectrometry and formation of covalent bonds with proteins resulting in shifting the isoform pattern. Protease inhibitors have been considered and investigated as additives in proteome research to prevent or slow down proteolytic processes and thereby provide a means of more sensitive detection of markers in blood.
Even though protein integrity has been shown to be maintained by addition of 15 commercially available protease inhibitors, the usefulness of protease inhibitors in overall protein stabilization of blood samples remains to be investigated in more detail. The presence of certain protease inhibitors in whole blood is toxic to live cells. Stressed, apoptotic or necrotic cells release substances, and it may be argued that this impacts the composition of serum or plasma until the cellular and the soluble factions of blood are separated. However careful selection of an appropriate protease inhibitor may solve this problem.
Even though protein integrity has been shown to be maintained by addition of 15 commercially available protease inhibitors, the usefulness of protease inhibitors in overall protein stabilization of blood samples remains to be investigated in more detail. The presence of certain protease inhibitors in whole blood is toxic to live cells. Stressed, apoptotic or necrotic cells release substances, and it may be argued that this impacts the composition of serum or plasma until the cellular and the soluble factions of blood are separated. However careful selection of an appropriate protease inhibitor may solve this problem.
Blood collection and specimen generation for Peptidomics analyses
The provision of adequate SOP’s is crucial to guarantee a high quality sample. Since in the discovery phase the number of samples to be analyzed is limited provision of high quality samples should be feasible. But more importantly this phase determines the outcome of all subsequent stages.
Disclaimer: Legal or ethical issues (e.g. importance of informed consents) or potential risks of phlebotomy (e.g. bleeding) are not covered.
These short lists provide only the basic procedures. You can download an in-depth description and a protocol from our website.
Blood collection
- favoured site of collection is the median cubital vein (easily found and accessed, comfortable for the patient)
- collect from fasting patients in the morning between 7-9 am (circadian rhythms)
- clean skin with an alcohol (2-propanol)
- allow alcohol to evaporate (danger of hemolysis, interference)
- apply tourniquet 3-4 inches above the site of venipuncture
- release as soon as blood begins flowing into the collection device (hemoconcentration)
- free flow has to be assured to avoid haemolysis
- centrifugation has to be started within 30 min after blood collection
Specimen generation
- centrifugation for 10 min at 2000 x g
- temperature should generally be 15-24 °C to prevent activation of platelets (unless recommended differently for distinct analytes like gastrin)
- a significant number of platelets (~25%) is still present in the sample, which requires an additional centrifugation step
- plasma is transferred into a second vial
- centrifugation for 15 min at 2500 x g at room temperature.
- supernatant is transferred in aliquots of 1.5 mL into cryo vials
Frequently made mistakes
- The blood sample tubes were put on ice or in a refrigerator.
- A cooling centrifuge was adjusted below room temperature.
- The centrifugation speed was wrong (e.g. rounds per minute were set instead of g-force).
- The removal of blood plasma by pipetting was done without proper caution (contamination with cells)
Further reading:
Specimen collection and handling: standardization of blood sample collection
Methods Mol Biol. 2008;428:35-42
Prerequisites for peptidomic analysis of blood samples: I. Evaluation of blood specimen qualities and determination of technical performance characteristics
Comb Chem High Throughput Screen. 2005 Dec;8(8):725-33
Specimen collection and handling: standardization of blood sample collection
Methods Mol Biol. 2008;428:35-42
Prerequisites for peptidomic analysis of blood samples: I. Evaluation of blood specimen qualities and determination of technical performance characteristics
Comb Chem High Throughput Screen. 2005 Dec;8(8):725-33